
A summer "third wave"?
UK Winter COVID-19 deaths closely tracked historical global patterns of winter respiratory infection. COVID-19 deaths fell last spring to near-zero. So why would there be a summer "third wave"?


DESPITE LAST WEEK’S denouncement by the Leader of Her Majesty’s Most Loyal Opposition of quoting Office for National Statistics COVID-19 data as “dangerous misinformation”,1 in this week’s newsletter we’ll be risking a look at ONS data to see what sense we can make of the pattern of winter COVID-19 deaths.
SARS-CoV-2—the virus that causes the COVID-19 disease in a small percentage of the population—is the seventh human coronavirus.2 The most common human coronaviruses are all winter seasonal respiratory infections. In the northern hemisphere, only 2.5% of endemic coronaviruse infections occur between the months of June and September. They begin increasing around September, peak in January, and return again to near zero in April.3
The seasonality of respiratory infection was studied by British doctor Robert Hope-Simpson, recipient of an OBE, the BMA Stuart Prize, the RCGP Kuenssberg prize and George Abercrombie award, and the VZV Foundation Gold Medal.4 He published his research in 1981.5
Hope-Simpson noted that epidemics of influenza occur within a distinctive annual cycle that alternates back and forth between the northern and southern hemispheres. However, although this cycle is anchored in the winter cold seasons in each hemisphere, epidemics also occur seasonally in parts of the globe (for example, India) where winter as a cold season does not occur. Hope-Simpson showed that it was the path of vertical solar radiation—which also causes reductions in winter both in temperature and vitamin D—not temperature itself, that was correlated with such epidemics. Perhaps most intriguingly, he showed that, before ubiquitous air travel, this seasonal influence appeared simultaneously in places lying at the same latitude whatever their longitude in a way that cannot easily be explained by the concept of direct human-to-human spread.
He summarised his findings in the following graphs, which are worth studying briefly:

Here in the UK, the all-cause death rate has returned back below its 5-year average, signalling the end of the 2020/21 winter seasonal respiratory infection period. So it’s now possible to superimpose the general features of the first full winter cycle of the newest coronavirus outbreak on Hope-Simpson’s “transequatorial” model of respiratory infection seasonality. The results are both interesting and potentially instructive.
For example, taking the historical data he used for influenza outbreaks in the northern temperate zone between 1964 and 1975, and superimposing UK deaths where COVID-19 is mentioned on the death certificate between July 2020 and April 2021, yields the following plot:6
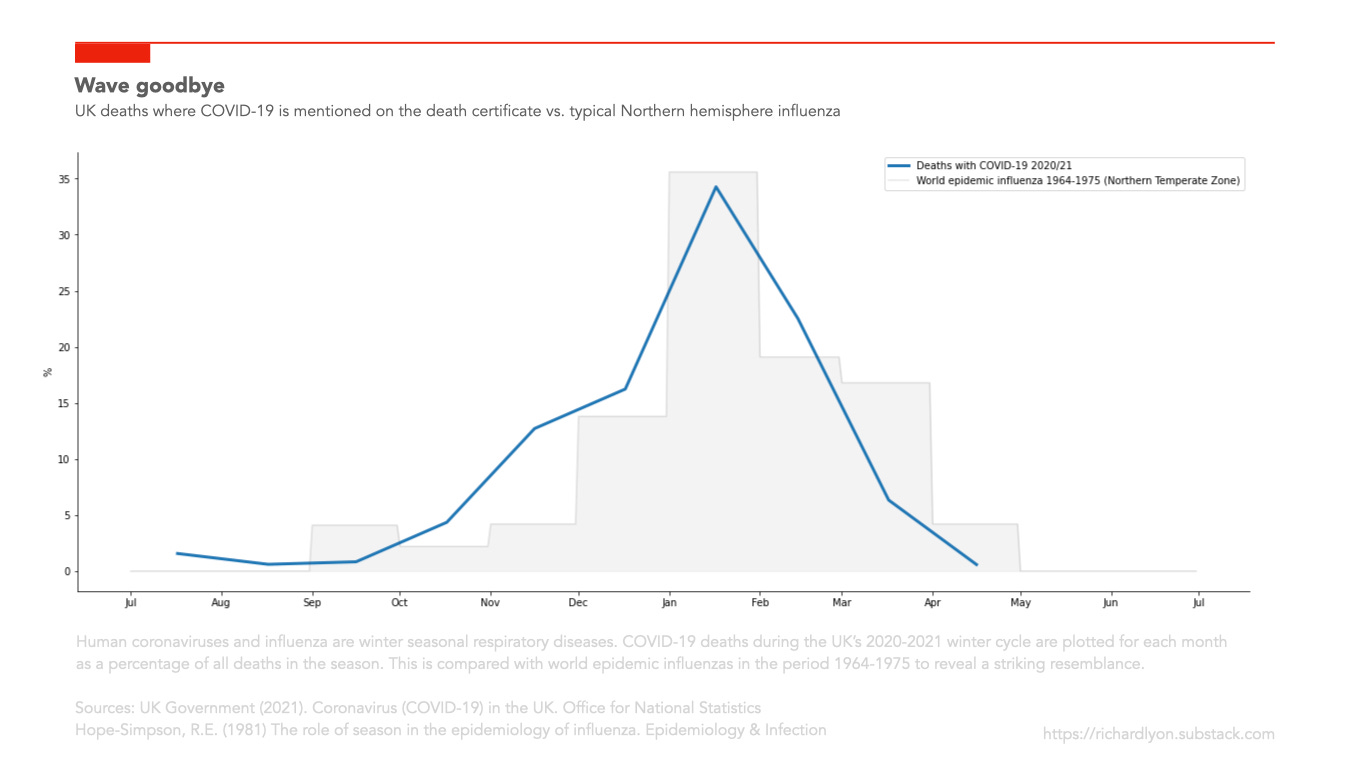
In both sets of data, around 35% of all infection occurs in January. The moderately higher proportion of COVID-19 deaths at the end of 2020 might be explained by the observation that SAR-CoV-2 had not yet reached endemic equilibrium, with correspondingly lower general immunity in the community—an outcome that we have spent over half a trillion pounds to delay through mandatory business closure and stay-at-home orders imposed on the healthy. The moderately lower proportion of COVID-19 deaths at the start of 2021 might be explained by the mass roll out of a specific and effective vaccine that was not carried out during the influenza epidemics. I don’t claim causality, but the correlation is certainly striking.
Another illustration of the Hope-Simpson seasonality model’s explanatory and possibly predictive power comes to us from current COVID-19 deaths in India. You are probably aware that these have begun rising. This is presented by those who make their livelihoods from cultivating fear and alarm about COVID-19 amongst the susceptible as evidence of a so-called “third wave”. They omit the context that India’s per-capita cumulative death currently stands at 6% of the UK’s,7 and attribute the cause of the current rise to ever more worrying “variants”. Inevitably, the only possible solution is the continuation of lockdowns in the UK, and of their speaker’s fees to explain this new danger to the public.

Yet, through the lens of the transequatorial model, the pattern of deaths is revealed as a repetition of the delayed rise, observed last year, as seasonal respiratory infections pass through the tropics from the northern hemisphere’s receding winter to the southern hemisphere’s approaching winter.
Wrong diagnosis, wrong cure
Until the 15th Century, the astrologers of the day assumed that the sky revolved around the Earth, and they drove themselves insane in their attempts to predict the paths that the planets traced in the night sky. Then Copernicus realised that the planets rotate around the Sun, the Church excommunicated Galileo for bringing it to everyone’s attention, and the elegance of modern celestial mechanics was revealed.
Today, this pattern of excommunication reinforced pseudoscience can be observed in lockdown theorists’ increasingly tortuous attempts to defend the claim that lockdowns have played a meaningful role in regulating the progress of a highly infectious virus through a society where up to two thirds of severe COVID-19 cases can occur in care homes and hospitals,8 fewer than half self-isolate after infection,9 everyone goes shopping, half travel daily to work10, children go to school, many finger and clamp to their faces contaminated apparel that traps, concentrates and causes its wearer to rebreath virus, bacteria and fungus, sweaty footballers hug and kiss each other even as our Queen sits in masked isolation during her husband’s burial, and everyone returns each night to close confinement with families in poorly ventilated homes where the relative rate of viral transmission is at its highest.
Their efforts to coerce into their belief system the progress of the infection as it settles into endemic equilibrium often generate busy, horoscope-like diagrams that would delight a 15th Century astrologer. Yet compare the complexity and, when you inspect them, the failure of such attempts to the straightforward observation that COVID-19—the next member of a family of diseases that are winter seasonal—went up when winter seasonal respiratory infection usually goes up, peaked when winter seasonal respiratory infection usually peaks, and went down when winter seasonal respiratory infection usually goes down.
The Law of Parsimony11 requires them to answer the questions: why introduce lockdowns as an additional explanatory factor, when seasonality appears sufficient? And why would a winter seasonal infection return this summer in a vaccinated, largely immune population when it didn’t last year in an unvaccinated, largely immunologically naive population?
They can’t, of course. So in the pseudoscience of lockdown, the questioner must be excommunicated; unlike other types of coronavirus, COVID-19 cannot be seasonal; the shape of the graph must be the product of lockdowns, not of seasonality (or even, if we are to believe the Prime Minister, of vaccines); the remarkable resemblance of the effect of lockdown to seasonality is entirely coincidental; we therefore cannot exclude the possibility of a “third wave”; lockdown must continue.
But in any contest between hallucination and reality, reality always wins. Last spring, in an unvaccinated population, and before the large number of healthy people who now have natural immunity had acquired it, COVID-19 in the UK fell to near-zero as we reopened society, and remained there until the winter respiratory infection cycle began again in September.
I expect it will again this year, whether they continue to destroy our health, our economy, and our children’s wellbeing or not.
Yorke, Harry. “Watch: ‘Get out of my pub’ - Sir Keir Starmer challenged by furious landlord over lockdown support”. The Telegraph. 19 April 2021 (link)
Huzar, Timothy. ‘Common coronaviruses appear to be highly seasonal’. Medical News Today. 17 April 2020. (link)
Hope-Simpson, Robert Edgar (1981), ‘The role of season in the epidemiology of influenza’, Epidemiology & Infection, 86 (1), 35-47. (link)
For the data and script used to generate this, see: https://github.com/richardjlyon/hopesimpson/tree/master
In noting that India’s per-capita death rate is only a small fraction of the UK’s, I wish to avoid the impression that I don’t regard the situation there, compounded by a relative lack of rural medical infrastructure, as being very sad. With a population of 1.34 billion, even low relative death rates translate into a large loss of human life, and the true death rate may well be underestimated. It’s also notable, however, that because of the catastrophic harm caused to the global economy by Western lockdown policies, poverty in India (the leading cause of death) has doubled in the last 12 months to 134 million, and of an estimated 1 million treatments worldwide of lethal tuberculosis that have not been carried out, a large number of those would have been in India.
McKeigue, Paul M, et al. (2021), ‘Relation of severe COVID-19 in Scotland to transmission-related factors and risk conditions eligible for shielding support: REACT-SCOT case-control study’, medRxiv (link)
Smith, Louise E, et al. (2021), ‘Adherence to the test, trace, and isolate system in the UK: results from 37 nationally representative surveys’, BMJ, n608. (link)
So, not only did Richard not seek permission, he is totally misquoting me.
I don't support lockdown, I merely seek to justify to myself, and to others, that the sacrifice being made to honour our social contract, is not killing people, and is working to genuinely save lives.
If it were not, I'd be shouting as loudly as Richard.
As to his observations of my work.
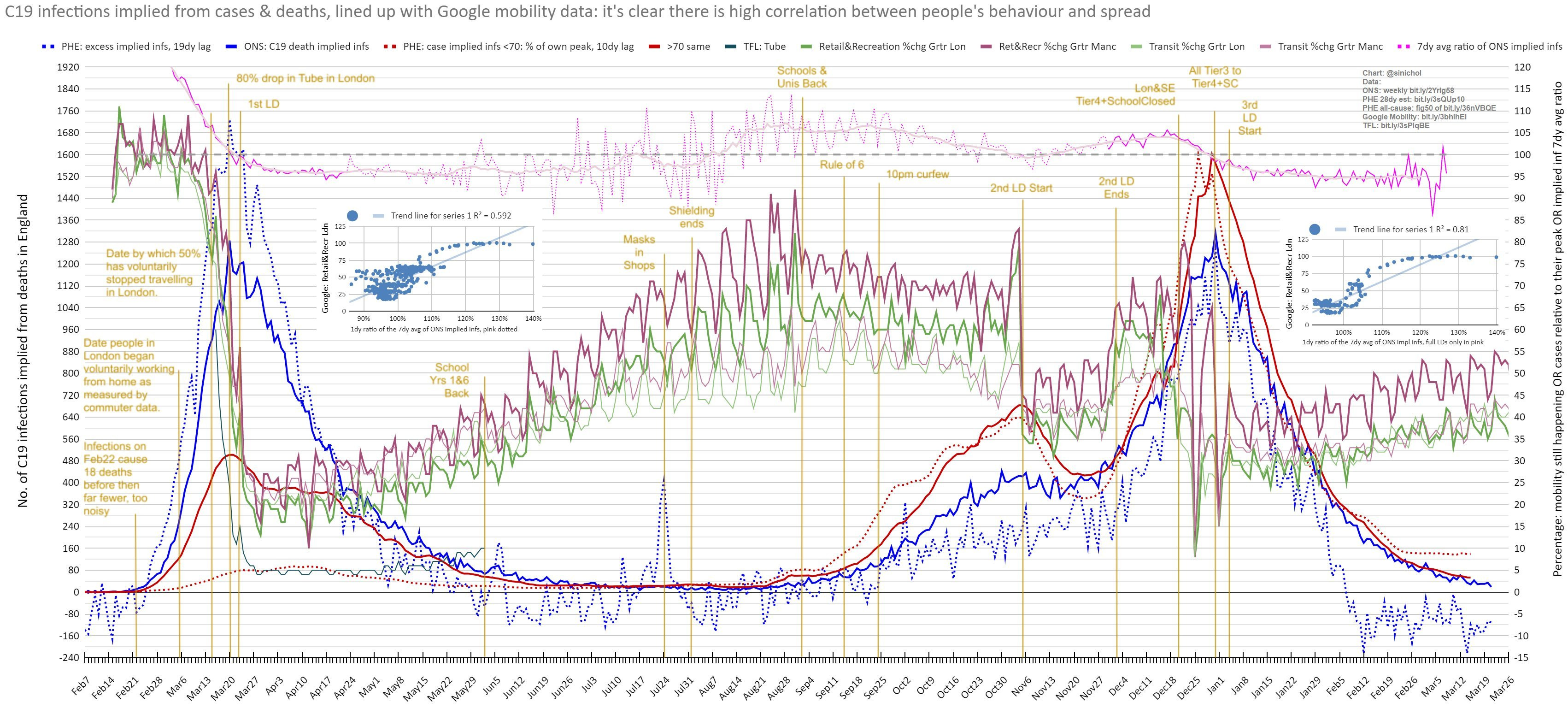
Beyond the mobility plateau to mid-May, where (per the pink lines at the top) the gradient of deaths is flat, and constant. As mobility lifts the rates of decline does slow.
This hits zero by mid Jul, then permanently makes it +ve in early Aug, getting very +ve by mid-late Aug.
All of this contrary to Richard's claim it is constant, and invariant to mobility.
As to Christmas, mobility clearly it was a superspreader event, with infections peaking by Dec28, beyond mobility shows people hunkered down, complied with Tier4 measures with schools closed, and that LD3, made little difference to movement patterns, as schools had been closed from Dec20, and this just kept this pattern of behaviour, and the constant decline in infections in place.
Nothing Richard says makes any sense.
His understanding of seasonality is also very flawed.
Seasonality starts after a few seasons of a new virus, when we finally hit the lower summer herd immunity threshold of a virus burning it out. For C19, from best R estimates, likely 60%, last summer NPIs had suppressed spread to 10%. Sure, summer behaviour patterns on top of this helped work against spread, and it getting colder into Sept/Oct did help drive up cases again, but the 2nd wave only took us to 25% spread, so his theory that hitting the natural summer HIT throttled spread, is for the birds.
Vaccinating the old, but not those <50, and lifting measures earlier in Sweden has led right now to their largest spike in cases to date. Sure, deaths are far lower, as vaccines are protecting those far more likely to die.
But, this does not change the reality of spread, and makes the argument that those unvaccinated <50 are anywhere near their summer HIT, with NPIs being lifted, just plain daft.
I don't say this to argue for further lockdowns. I support lifting measures now.
I simply say it so that we all understand the risk trade off we are making with the current policy choice. That being that spread is very likely to be larger than it has been so far, if we can't vaccinate those <50 asap, and that will carry with it the risk of a "mosh pit" that is very likely to generate another home grown variant that might then beat vaccines in our vulnerable cohort this coming winter.
I say it simply so we are correctly aware of the trade off we are making.
All his other noise, and insults, are just there to hide his poor analysis.